A Meta-Analysis of Mobile Health and Risk Reduction in Patients with Diabetes Mellitus: Challenge and Opportunity
Dr Longjian Liu PHD1, Stella-Maris Ogwu MPH1,2
1Department of Epidemiology and Biostatistics, Drexel University School of Public Health, Philadelphia, USA, 2Opening Doors for Health Disparity Training Porgram, Drexel University School of Public Health, Philadelphia, USA Corresponding Author: longjian.liu@drexel.edu
Journal MTM 1:3:17-24, 2012
DOI:10.7309/jmtm.18
Purpose: To examine scientific evidence on the effectiveness of mobile phone technology in Diabetes Mellitus (DM) care management.
Methods: A systematic review was conducted through literature searches from three electronic databases and was restricted to English-language articles published between January 2002 and March 2012. Studies that used mobile phone intervention and reported changes in diet, physical activity, and blood glucose and /or glycosylated hemoglobin (HbA1c) levels were retrieved. A meta-analysis was conducted for studies with HbA1c measures.
Results: More than 50 articles were screened. Of them, 15 met the review criteria. Of the 15, study sample sizes ranged from 12 to 130 participants aged 8 to 70 years old. Duration of intervention ranged from 1 to 12 months. Overall, significant improvements were observed in blood glucose and/or HbA1c concentration, adherence to medication, healthy lifestyle, and self-efficacy. Twelve of 15 trials, which had serum HbA1c measures, showed an average 0.39% (95%CI: -0.067, -0.721) HbA1c reduction from studies with pre- to post-tests (p=0.018).
Conclusion: Findings from the study provide the evidence that health reminders, disease monitoring and management, and education through mobile phone technology may significantly help improve glycaemic control patients with DM.
Introduction
There has been a rapid escalation in the rate by which mobile technology has been adopted in the United States and globally1Atienza AA and Patrick K. Mobile health: the killer app for cyberinfrastructure and consumer health. Am. J. Prev. Med. 2011;40,(5 Suppl 2):S151-3., 2Blumberg SJ, Luke JV, Ganesh N, Davern ME, Boudreaux MH and Soderberg K. Wireless substitution: state-level estimates from the National Health Interview Survey, January 2007-June 2010. Natl. Health. Stat. Report 2011;(39),(39):1-26, 28.. More recently, as of June 2011, the U.S had an estimated 331.6 million wireless subscribers (Cellular Telecommunications & Internet Association (CTIA), 2011) and 4.6 billion mobile cellular subscriptions worldwide3International Telecommunication Union. World Telecommunication/ICT Development Report 2010: Monitoring the Wsis targets - A mid-term review: http://www.uis.unesco.org/Communication/Documents/WTDR2010_e.pdf (Accessed on May 16, 2012)..
As mobile phone technology continues to expand and electronic medical and personal health records (PHRs) grow simultaneously, mobile phones will become increasingly important in the strategic implementation of chronic disease management 1Atienza AA and Patrick K. Mobile health: the killer app for cyberinfrastructure and consumer health. Am. J. Prev. Med. 2011;40,(5 Suppl 2):S151-3., 4Blake H. Mobile phone technology in chronic disease management. Nurs. Stand. 2008;23,(12):43-46.. Research evidence suggests that mobile phone technology may be beneficial in diet and weight management 5Wang DH, Kogashiwa M and Kira S. Development of a new instrument for evaluating individuals' dietary intakes. J. Am. Diet. Assoc. 2006;106,(10):1588-1593., 6Kubota A, Fujita M and Hatano Y. Development and effects of a health promotion program utilizing the mail function of mobile phones. Nihon Koshu Eisei Zasshi. 2004;51,(10):862-873., physical activity involvement 7Hurling R, Catt M, Boni MD, Fairley BW, Hurst T, Murray P, Richardson A and Sodhi JS. Using internet and mobile phone technology to deliver an automated physical activity program: randomized controlled trial. J. Med. Internet Res. 2007;9,(2):e7., 8Consolvo, S., Everitt, K., Smith, I., & Landay, J. A. Design requirements for technologies that encourage physical activity: http://dub.washington.edu/djangosite/media/papers/paper0552-consolvo.pdf (Accessed on May 16, 2012)., asthma control 9Britto MT, Munafo JK, Schoettker PJ, Vockell AL, Wimberg JA and Yi MS. Pilot and feasibility test of adolescent-controlled text messaging reminders. Clin. Pediatr. (Phila) 2012;51,(2):114-121., 10Anhoj J and Moldrup C. Feasibility of collecting diary data from asthma patients through mobile phones and SMS (short message service): response rate analysis and focus group evaluation from a pilot study. J. Med. Internet Res. 2004;6,(4):e42., and diabetes management 11Faridi Z, Liberti L, Shuval K, Northrup V, Ali A and Katz DL. Evaluating the impact of mobile telephone technology on type 2 diabetic patients' self-management: the NICHE pilot study. J. Eval. Clin. Pract. 2008;14,(3):465-469., 12Vahatalo, M. A, Virtamo, H. E., Viikari, J. S., and Ronnemaa, T. Cellular phone transferred self-blood glucose monitoring: prerequisites for positive outcome. Practical Diabetes International 2004;21,(5):192-194..
Diabetes Mellitus (DM) is a highly prevalent chronic disease in the United States and in the world 13-1513. Liu L. Social connections, diabetes mellitus, and risk of mortality among white and African-American adults aged 70 and older: an eight-year follow-up study. Ann. Epidemiol. 2011;21,(1):26-33.
14. Liu L. Changes in cardiovascular hospitalization and comorbidity of heart failure in the United States: findings from the National Hospital Discharge Surveys 1980-2006. Int. J. Cardiol. 2011;149,(1):39-45.
15. L. Liu, X. Yin, S. Morrissey. Global variability in diabetes mellitus and its association with body weight and primary healthcare support in 49 low- and middle-income developing countries: http://onlinelibrary.wiley.com/doi/10.1111/j.1464-5491.2011.03549.x/abstract (Accessed on 12/06, 2011).. Although several methods of patient care have been well established to improve clinical profile and complications associated with DM, effectiveness of novel interventions remains to be evaluated 16Liang X, Wang Q, Yang X, Cao J, Chen J, Mo X, Huang J, Wang L and Gu D. Effect of mobile phone intervention for diabetes on glycaemic control: a meta-analysis. Diabet. Med. 2011;28,(4):455-463..
The purpose of this review is to identify the impact of mobile phone technology interventions on DM care and patient outcomes, recognize potential challenges and limitations associated with performing healthcare practice and conducting research in this field, and examine practical ways of incorporating mobile phone technology in DM management.
Methods
Data sources
Electronic literature searches were conducted extensively to identify all eligible observational and randomized controlled clinical trials. Searches were performed on three major databases including PubMed, Ovid MEDLINE, and Google scholar using combined terms of ‘diabetes’, ‘diabetes mellitus’, ‘cellular phone’ ‘mobile phone’, and ‘text message’. In addition, manual searches were completed by screening the bibliographies and citations of published articles. The search was restricted to English-language articles published between January 2002 and March 2012.
Eligibility criteria
Studies were selected for the review based on the following criteria: (1) participants had clinically diagnosis of DM (either type II or type I); (2) the study evaluated use of mobile phones for DM self management; (3) effect was measured in the process or outcome of DM care; and (4) the studies with designs of randomized controlled trial, quasi-randomized trial, crossover randomized clinical trial, or observational cohort studies. Studies were excluded if (1) they were case reports, and (2) if other communication technologies such as the Internet, e-mail, or video messaging were used as the primary mode of communication instead of mobile phone technology.
Data extraction
Relevant datafrom each eligible published paper were extracted into a structured spreadsheet. Authors, year of publication, study setting, sample size, study design, age group, race, duration of intervention, outcomes, method of self-management, intervention details, and reported results were reviewed.
Meta-analysis
Studies with a randomized controlled trial design and having pre- and post-intervention measures of serum HbA1c concentration were further analyzed using meta-analysis random effect modeling approach to quantitatively estimate the overall effect from multiple studies.
Results
Characteristics of included studies
In the initial review, more than 50 articles were screened. After excluding studies that did not meet the eligibility criteria, 15 studies were reviewed intensively. Of them, studies took place in several countries including Korea 17Kim HS and Jeong HS. A nurse short message service by cellular phone in type-2 diabetic patients for six months. J. Clin. Nurs. 2007;16,(6):1082-1087., 17-2017. Kim HS and Jeong HS. A nurse short message service by cellular phone in type-2 diabetic patients for six months. J. Clin. Nurs. 2007;16,(6):1082-1087.
18.Kim CS, Park SY, Kang JG, Lee SJ, Ihm SH, Choi MG and Yoo HJ. Insulin dose titration system in diabetes patients using a short messaging service automatically produced by a knowledge matrix. Diabetes Technol. Ther. 2010;12,(8):663-669.
19.Yoon KH and Kim HS. A short message service by cellular phone in type 2 diabetic patients for 12 months. Diabetes Res. Clin. Pract. 2008;79,(2):256-261.
20.Cho JH, Lee HC, Lim DJ, Kwon HS and Yoon KH. Mobile communication using a mobile phone with a glucometer for glucose control in Type 2 patients with diabetes: as effective as an Internet-based glucose monitoring system. J. Telemed. Telecare 2009;15,(2):77-82.
, U.S 11Faridi Z, Liberti L, Shuval K, Northrup V, Ali A and Katz DL. Evaluating the impact of mobile telephone technology on type 2 diabetic patients' self-management: the NICHE pilot study. J. Eval. Clin. Pract. 2008;14,(3):465-469., 21-2321. Arsand E, Tatara N, Ostengen G and Hartvigsen G. Mobile phone-based self-management tools for type 2 diabetes: the few touch application. J. Diabetes Sci. Technol. 2010;4,(2):328-336.
22. Dick JJ, Nundy S, Solomon MC, Bishop KN, Chin MH and Peek ME. Feasibility and usability of a text message-based program for diabetes self-management in an urban African-American population. J. Diabetes Sci. Technol. 2011;5,(5):1246-1254.
23. Fischer HH, Moore SL, Ginosar D, Davidson AJ, Rice-Peterson CM, Durfee MJ, Mackenzie TD, Estacio RO and Steele AW. Care by cell phone: text messaging for chronic disease management. Am. J. Manag. Care 2012;18,(2):e42-7.
, Austria 24Rami B, Popow C, Horn W, Waldhoer T and Schober E. Telemedical support to improve glycemic control in adolescents with type 1 diabetes mellitus. Eur. J. Pediatr. 2006;165,(10):701-705., Finland 12, Iran 25Zolfaghari M, Mousavifar SA, Pedram S and Haghani H. The impact of nurse short message services and telephone follow-ups on diabetic adherence: which one is more effective? J. Clin. Nurs. 2012;., U.K 26-2926. Farmer A, Gibson O, Hayton P, Bryden K, Dudley C, Neil A and Tarassenko L. A real-time, mobile phone-based telemedicine system to support young adults with type 1 diabetes. Inform. Prim. Care. 2005;13,(3):171-177.
27. Farmer AJ, Gibson OJ, Dudley C, Bryden K, Hayton PM, Tarassenko L and Neil A. A randomized controlled trial of the effect of real-time telemedicine support on glycemic control in young adults with type 1 diabetes (ISRCTN 46889446). Diabetes Care 2005;28,(11):2697-2702.
28. Franklin VL, Waller A, Pagliari C and Greene SA. A randomized controlled trial of Sweet Talk, a text-messaging system to support young people with diabetes. Diabet. Med. 2006;23,(12):1332-1338.
29. Turner J, Larsen M, Tarassenko L, Neil A and Farmer A. Implementation of telehealth support for patients with type 2 diabetes using insulin treatment: an exploratory study. Inform. Prim. Care. 2009;17,(1):47-53., and multi center (Italy, England, and Spain)30Rossi MC, Nicolucci A, Di Bartolo P, Bruttomesso D, Girelli A, Ampudia FJ, Kerr D, Ceriello A, Mayor Cde L, Pellegrini F, Horwitz D and Vespasiani G. Diabetes Interactive Diary: a new telemedicine system enabling flexible diet and insulin therapy while improving quality of life: an open-label, international, multicenter, randomized study. Diabetes Care 2010;33,(1):109-115.. Patients were recruited from primary clinics, tertiary hospitals and community settings. Figure 1 shows the selection of studies.
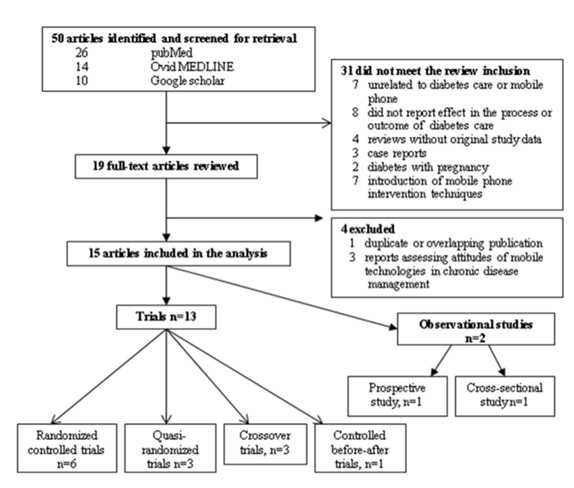
Figure 1 – Papers selected for the systematic review of mobile phone technologies involving diabetes care and management
Of the 15 studies, 2 were observational studies (one cross-sectional and one prospective cohort study) and the other 13 were randomized controlled trials. The minimum duration of intervention in these studies was 1 month and maximum of 12 months. Sample size ranged from 12 to 130 participants at the end of the follow-up period and all studies included both males and females. Gender was distributed almost equally in all the studies. Participants were aged 8-70 years old. Five studies examined patients with Type 1 DM, eight studies observed patients with Type 2 DM, and two studies included patients with both Type 1 and Type 2 DM.
Approach of mobile phone intervention
Mobile phone intervention in the included studies showed a wide range of technological innovations. Three of the studies developed software or an application programmed for diabetes care management 11Faridi Z, Liberti L, Shuval K, Northrup V, Ali A and Katz DL. Evaluating the impact of mobile telephone technology on type 2 diabetic patients' self-management: the NICHE pilot study. J. Eval. Clin. Pract. 2008;14,(3):465-469., 21Arsand E, Tatara N, Ostengen G and Hartvigsen G. Mobile phone-based self-management tools for type 2 diabetes: the few touch application. J. Diabetes Sci. Technol. 2010;4,(2):328-336., 28Franklin VL, Waller A, Pagliari C and Greene SA. A randomized controlled trial of Sweet Talk, a text-messaging system to support young people with diabetes. Diabet. Med. 2006;23,(12):1332-1338.. The others used both mobile phone technology and Internet to provide support for self-monitoring blood glucose, continuous education, reinforcement of diet, exercise, and medication adjustment 12Vahatalo, M. A, Virtamo, H. E., Viikari, J. S., and Ronnemaa, T. Cellular phone transferred self-blood glucose monitoring: prerequisites for positive outcome. Practical Diabetes International 2004;21,(5):192-194., 17Kim HS and Jeong HS. A nurse short message service by cellular phone in type-2 diabetic patients for six months. J. Clin. Nurs. 2007;16,(6):1082-1087., 17-2017. Kim HS and Jeong HS. A nurse short message service by cellular phone in type-2 diabetic patients for six months. J. Clin. Nurs. 2007;16,(6):1082-1087.
18. Kim CS, Park SY, Kang JG, Lee SJ, Ihm SH, Choi MG and Yoo HJ. Insulin dose titration system in diabetes patients using a short messaging service automatically produced by a knowledge matrix. Diabetes Technol. Ther. 2010;12,(8):663-669.
19. Yoon KH and Kim HS. A short message service by cellular phone in type 2 diabetic patients for 12 months. Diabetes Res. Clin. Pract. 2008;79,(2):256-261.
20. Cho JH, Lee HC, Lim DJ, Kwon HS and Yoon KH. Mobile communication using a mobile phone with a glucometer for glucose control in Type 2 patients with diabetes: as effective as an Internet-based glucose monitoring system. J. Telemed. Telecare 2009;15,(2):77-82..
Among the 15 included studies, 12 used a mobile phone Short Message Service (SMS) to deliver blood glucose test results and self-management information. These studies adopted a short message service alone, or SMS combined with other intervention strategies, which included transmitting self-monitored blood glucose to mobile phone via a Bluetooth wireless link. One study 26Farmer A, Gibson O, Hayton P, Bryden K, Dudley C, Neil A and Tarassenko L. A real-time, mobile phone-based telemedicine system to support young adults with type 1 diabetes. Inform. Prim. Care. 2005;13,(3):171-177., combined mobile phone with clinical visits that consisted of medical advice and structured counseling from a diabetes specialist nurse in response to real-time blood glucose test. The combined intervention appeared achieving a greater reduction in HbA1c than isolated mobile phone intervention.
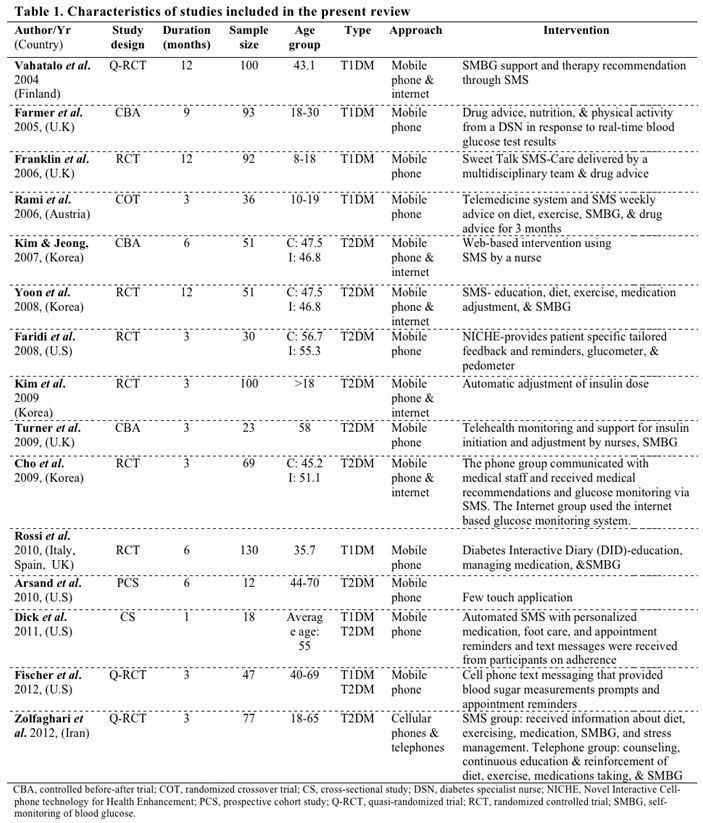
Table 1 summarizes the key features of studies included in the systematic review. Outcome measures varied across individual studies, including HbA1c concentration, insulin and lipid profile levels, changes in body weight, blood pressure values, self-efficacy, and perception of the use of mobile phone technology.
Effects of intervention
Glycosylated hemoglobin (HbA1c) levels were measured in 12 studies (Fig 2). The effects of the intervention in each study was calculated as the difference in the mean percentage change of HbA1c value from pre-intervention to post-intervention in the intervention and control groups. The minimum difference reported at the end of the study period in the intervention group was -0.1 (6.4% pretest to 6.3% at 3 months) while the maximum difference was -2.4 (9.8% pretest to 7.4% at 3 months). Ten studies showed lower HbA1c levels among participants in the intervention group at the end of the intervention, although only seven 17Kim HS and Jeong HS. A nurse short message service by cellular phone in type-2 diabetic patients for six months. J. Clin. Nurs. 2007;16,(6):1082-1087., 19Yoon KH and Kim HS. A short message service by cellular phone in type 2 diabetic patients for 12 months. Diabetes Res. Clin. Pract. 2008;79,(2):256-261., 20Cho JH, Lee HC, Lim DJ, Kwon HS and Yoon KH. Mobile communication using a mobile phone with a glucometer for glucose control in Type 2 patients with diabetes: as effective as an Internet-based glucose monitoring system. J. Telemed. Telecare 2009;15,(2):77-82., 25Zolfaghari M, Mousavifar SA, Pedram S and Haghani H. The impact of nurse short message services and telephone follow-ups on diabetic adherence: which one is more effective? J. Clin. Nurs. 2012;., 27Farmer AJ, Gibson OJ, Dudley C, Bryden K, Hayton PM, Tarassenko L and Neil A. A randomized controlled trial of the effect of real-time telemedicine support on glycemic control in young adults with type 1 diabetes (ISRCTN 46889446). Diabetes Care 2005;28,(11):2697-2702., 28Franklin VL, Waller A, Pagliari C and Greene SA. A randomized controlled trial of Sweet Talk, a text-messaging system to support young people with diabetes. Diabet. Med. 2006;23,(12):1332-1338., 30Rossi MC, Nicolucci A, Di Bartolo P, Bruttomesso D, Girelli A, Ampudia FJ, Kerr D, Ceriello A, Mayor Cde L, Pellegrini F, Horwitz D and Vespasiani G. Diabetes Interactive Diary: a new telemedicine system enabling flexible diet and insulin therapy while improving quality of life: an open-label, international, multicenter, randomized study. Diabetes Care 2010;33,(1):109-115. reported significant reduction in HbA1c levels (p < 0.05). Meta-analysis suggests that during an average follow-up of 6.3 years, an overall net effect of HbA1c reduction of the 12 studies in intervention groups was 0.39% (95%CI: -0.067, -0.72, p=0.018) after taking off the reduction in control groups.
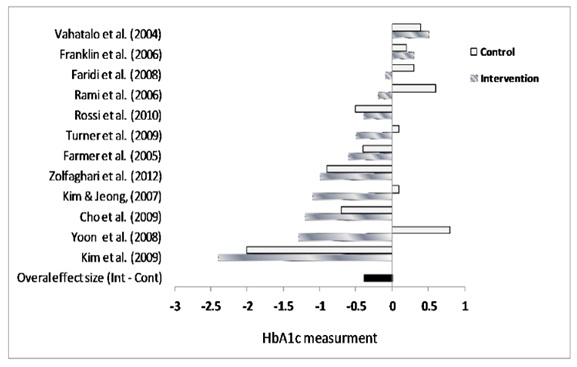
Figure 2 – Meta-analysis for studies with HbA1c measures
Discussion
Maintaining health lifestyle in patients with DM is fundamental to their health status and welfare. Mobile phone technology may be essential in interventions that target behavioral and lifestyle changes, particularly, those associated with chronic diseases management. Our study reviewed fifteen studies that assessed the effect of mobile phone interventions on the self monitoring and management of DM provides evidence that there is a significant effect on DM management using mobile technique. This result is consistent with existing literature 17-1917. Kim HS and Jeong HS. A nurse short message service by cellular phone in type-2 diabetic patients for six months. J. Clin. Nurs. 2007;16,(6):1082-1087.
18. Kim CS, Park SY, Kang JG, Lee SJ, Ihm SH, Choi MG and Yoo HJ. Insulin dose titration system in diabetes patients using a short messaging service automatically produced by a knowledge matrix. Diabetes Technol. Ther. 2010;12,(8):663-669.
19. Yoon KH and Kim HS. A short message service by cellular phone in type 2 diabetic patients for 12 months. Diabetes Res. Clin. Pract. 2008;79,(2):256-261..
The main contribution of the present review provides the most recent evidence of mHealth studies, and the findings are based on studies from different countries. Among the reviewed studies, most applied randomized controlled designs, which enhanced the comparability of the outcomes. Also, most studies applied quantitative measures of key outcomes, including HbA1c, weight loss and serum glucose concentration measurement.
Despite the strengths of mobile phone technology use, several potential limitations should be kept in mind when interpreting these results. First, although findings from the reviewed studies showed promise in mobile phone use and improvement of DM management, some of these studies had small sample sizes. Therefore, future studies that utilize large sample size are needed to determine whether the increased patient-providers’ communication via mHealth have significant impacts on clinical outcomes and public health. Secondly, it is unknown what kind of modalities of mobile technology (SMS, mobile phone calls, application, etc) play a better role in improving outcomes in patients with DM. Thirdly, since most studies had a short period of intervention, the long-term effects of mHealth are still unclear. Fourthly, the current review paper is done by the authors in searching for the relevant literatures. We may have missed some papers during the search. If any, it will cause potential selection bias. Further studies should be continued to confirm the findings. Lastly, as with all systematic reviews, the present study is subject to publication bias 31Cole-Lewis H and Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol. Rev. 2010;32,(1):56-69..
It should be noted that our present study aims to review the studies in the last decade and to evaluate the feasibility of using mobile phone technology to promote patients’ DM management and improve healthy lifestyle. It is clear that although mHealth techniques may offer new opportunities in disease control, we still face several challenges. First, the application of mHealth is a new approach in real-world practice. Most studies are still in the exploratory stages. Therefore, it is essential to find the link between practice and scientific knowledge, which come from studies with vigorous study designs and a large-scale sample size. Secondly, continuous adherence and compliance to mobile phone technology in DM management is crucial to the outcomes. The mobile phone use intervention relies heavily on behavioral change theory. In other words, the innovation is based on a patient’s willingness to fully participate in every aspect of the intervention. Thus, the intervention may not be suitable for all patients with DM, such as those who may have difficulties operate smart phone. Several studies observed that some patients withdrew from an intervention study due to the inconvenience of using the assigned mobile phones on a regular day-to-day basis. Therefore, findings observed in most studies are based on participants who may be highly motivated 1Atienza AA and Patrick K. Mobile health: the killer app for cyberinfrastructure and consumer health. Am. J. Prev. Med. 2011;40,(5 Suppl 2):S151-3.. Thirdly, mobile phone technology raises important questions about how to protect patients with DM while simultaneously promoting its development and implementation 1Atienza AA and Patrick K. Mobile health: the killer app for cyberinfrastructure and consumer health. Am. J. Prev. Med. 2011;40,(5 Suppl 2):S151-3.. This includes challenges associated with privacy and confidentiality of information collected and stored by mobile devices and/or transmitted to cyber infrastructure databases. For notification and intervention purposes, additional privacy and confidentiality concerns arise when sending health-related data to mobile devices 32Kang BS and Ko IY. Effective route maintenance and restoration schemes in mobile ad hoc networks. Sensors (Basel) 2010;10,(1):808-821.. For example, interventions can be interrupted and privacy may be breached if the mobile phone is lost or stolen. However, similar limitations are present with other communication modes (e.g., postal mail or emails may be delivered to the wrong address) 31Cole-Lewis H and Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol. Rev. 2010;32,(1):56-69.. It is important to ensure that information gathered and transmitted via mobile devices remains secure 1Atienza AA and Patrick K. Mobile health: the killer app for cyberinfrastructure and consumer health. Am. J. Prev. Med. 2011;40,(5 Suppl 2):S151-3.. Fourthly, although mobile phone technology promises unprecedented opportunities to reach DM patients anytime and anywhere, mHealth interventions may result in the marginalization of certain populations, such as illiterates or those without access to a mobile phone 31Cole-Lewis H and Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol. Rev. 2010;32,(1):56-69.. These drawbacks may greatly affect the impact of such interventions in such population. In the United States, mobile handset ownership differs among different ethnic groups and access is lower among those with lower socioeconomic status (defined as those with less than a high school graduate). Similarly, evidence points to disparity between younger and older patients 1Atienza AA and Patrick K. Mobile health: the killer app for cyberinfrastructure and consumer health. Am. J. Prev. Med. 2011;40,(5 Suppl 2):S151-3.. Possible explanations for this disparity might be related to age, urban and rural, and economy; although neither of these reasons has been definitively determined. Fifthly, mobile phones and Internet technology are advancing rapidly and are ubiquitously available worldwide 16Liang X, Wang Q, Yang X, Cao J, Chen J, Mo X, Huang J, Wang L and Gu D. Effect of mobile phone intervention for diabetes on glycaemic control: a meta-analysis. Diabet. Med. 2011;28,(4):455-463.. However, the costs to participants and healthcare providers are still difficult to estimate. Moreover, the question remains as to who will be responsible for covering the attributable costs of this innovation in the real world. Unfortunately, only three studies 24Rami B, Popow C, Horn W, Waldhoer T and Schober E. Telemedical support to improve glycemic control in adolescents with type 1 diabetes mellitus. Eur. J. Pediatr. 2006;165,(10):701-705., 28Franklin VL, Waller A, Pagliari C and Greene SA. A randomized controlled trial of Sweet Talk, a text-messaging system to support young people with diabetes. Diabet. Med. 2006;23,(12):1332-1338., 30Rossi MC, Nicolucci A, Di Bartolo P, Bruttomesso D, Girelli A, Ampudia FJ, Kerr D, Ceriello A, Mayor Cde L, Pellegrini F, Horwitz D and Vespasiani G. Diabetes Interactive Diary: a new telemedicine system enabling flexible diet and insulin therapy while improving quality of life: an open-label, international, multicenter, randomized study. Diabetes Care 2010;33,(1):109-115. in this review had cost/benefit analysis information, in which they reported that self-monitoring and management of diabetes via mobile phone technology would be cost-effective at approximately €4/month, 2 pence/text, and €1.4/month respectively. Nevertheless, the applicability of mobile technology in low resources settings is still questionable in terms of its overall cost (phone, internet and operation). Furthermore, patients with DM are disproportionately distributed in those with low socioeconomic status. The application of mobile technology calls for healthcare system and health policy reforms to meet an urgent need of an increasing trend of DM in the United States and worldwide13Liu L. Social connections, diabetes mellitus, and risk of mortality among white and African-American adults aged 70 and older: an eight-year follow-up study. Ann. Epidemiol. 2011;21,(1):26-33., 15L. Liu, X. Yin, S. Morrissey. Global variability in diabetes mellitus and its association with body weight and primary healthcare support in 49 low- and middle-income developing countries: http://onlinelibrary.wiley.com/doi/10.1111/j.1464-5491.2011.03549.x/abstract (Accessed on 12/06, 2011)., 33Kabadi SM, Lee BK and Liu L. Joint Effects of Obesity and Vitamin D Insufficiency on Insulin Resistance and Type 2 Diabetes: Results from the NHANES 2001-2006. Diabetes Care 2012, Epub ahead of print., 34Liu L and Nunez AE. Cardiometabolic syndrome and its association with education, smoking, diet, physical activity, and social support: findings from the Pennsylvania 2007 BRFSS Survey. J. Clin. Hypertens. (Greenwich) 2010;12,(7):556-564..
Conclusion
The results from the present study indicate significant improvements in gylcaemic control and self-management with mobile phone intervention methods for DM care. Most reviewed studies demonstrated the promise of mHealth to aid patients and to reduce HbA1c by the use of mobile phone technology. Further research with a longer duration and larger sample size is needed to examine several key issues including the benefits of mHealth interventions for patients and healthcare providers’ perceptions, and how mHealth integrating appropriately into healthcare practice, and the cost effectiveness of intervention in improving self-management in patents with diabetes.
Acknowledgements
No conflict of interest to report.Authors’ contribution: Longjian Liu, MD, PhD, MSc, contributed to the study design, analysis approach, reviewed, edited and finalized the manuscript. Stella-Maris Ogwu, MPH, participated in the study design, contributed to data collection, analysis and drafted the manuscript when she took the Opening Doors Health Disparities Training Program (February – June, 2012), supervised by Dr. L Liu, at Drexel University School of Public Health. Stella-Maris Ogwu was supported by a grant from the National Institute of Health for the Opening Doors Health Disparities Training Program at Drexel University School of Public Health (NIH Grant # R25 MD006792-01). The present study was presented in abstract form (poster) by SM Ogwu and L Liu at 2012 Public Health Poster Session of the College of Physicians of Philadelphia (May 16).
References
1. Atienza AA and Patrick K. Mobile health: the killer app for cyberinfrastructure and consumer health. Am. J. Prev. Med. 2011;40,(5 Suppl 2):S151-3. ![]()
2. Blumberg SJ, Luke JV, Ganesh N, Davern ME, Boudreaux MH and Soderberg K. Wireless substitution: state-level estimates from the National Health Interview Survey, January 2007-June 2010. Natl. Health. Stat. Report 2011;(39),(39):1-26, 28.
3. International Telecommunication Union. World Telecommunication/ICT Development Report 2010: Monitoring the Wsis targets – A mid-term review: http://www.uis.unesco.org/Communication/Documents/WTDR2010_e.pdf (Accessed on May 16, 2012).
4. Blake H. Mobile phone technology in chronic disease management. Nurs. Stand. 2008;23,(12):43-46.
5. Wang DH, Kogashiwa M and Kira S. Development of a new instrument for evaluating individuals’ dietary intakes. J. Am. Diet. Assoc. 2006;106,(10):1588-1593. ![]()
6. Kubota A, Fujita M and Hatano Y. Development and effects of a health promotion program utilizing the mail function of mobile phones. Nihon Koshu Eisei Zasshi. 2004;51,(10):862-873.
7. Hurling R, Catt M, Boni MD, Fairley BW, Hurst T, Murray P, Richardson A and Sodhi JS. Using internet and mobile phone technology to deliver an automated physical activity program: randomized controlled trial. J. Med. Internet Res. 2007;9,(2):e7. ![]()
8. Consolvo, S., Everitt, K., Smith, I., & Landay, J. A. Design requirements for technologies that encourage physical activity: http://dub.washington.edu/djangosite/media/papers/paper0552-consolvo.pdf (Accessed on May 16, 2012).
9. Britto MT, Munafo JK, Schoettker PJ, Vockell AL, Wimberg JA and Yi MS. Pilot and feasibility test of adolescent-controlled text messaging reminders. Clin. Pediatr. (Phila) 2012;51,(2):114-121. ![]()
10. Anhoj J and Moldrup C. Feasibility of collecting diary data from asthma patients through mobile phones and SMS (short message service): response rate analysis and focus group evaluation from a pilot study. J. Med. Internet Res. 2004;6,(4):e42. ![]()
11. Faridi Z, Liberti L, Shuval K, Northrup V, Ali A and Katz DL. Evaluating the impact of mobile telephone technology on type 2 diabetic patients’ self-management: the NICHE pilot study. J. Eval. Clin. Pract. 2008;14,(3):465-469. ![]()
12. Vahatalo, M. A, Virtamo, H. E., Viikari, J. S., and Ronnemaa, T. Cellular phone transferred self-blood glucose monitoring: prerequisites for positive outcome. Practical Diabetes International 2004;21,(5):192-194. ![]()
13. Liu L. Social connections, diabetes mellitus, and risk of mortality among white and African-American adults aged 70 and older: an eight-year follow-up study. Ann. Epidemiol. 2011;21,(1):26-33. ![]()
14. Liu L. Changes in cardiovascular hospitalization and comorbidity of heart failure in the United States: findings from the National Hospital Discharge Surveys 1980-2006. Int. J. Cardiol. 2011;149,(1):39-45. ![]()
15. L. Liu, X. Yin, S. Morrissey. Global variability in diabetes mellitus and its association with body weight and primary healthcare support in 49 low- and middle-income developing countries: http://onlinelibrary.wiley.com/doi/10.1111/j.1464-5491.2011.03549.x/abstract (Accessed on 12/06, 2011).
16. Liang X, Wang Q, Yang X, Cao J, Chen J, Mo X, Huang J, Wang L and Gu D. Effect of mobile phone intervention for diabetes on glycaemic control: a meta-analysis. Diabet. Med. 2011;28,(4):455-463. ![]()
17. Kim HS and Jeong HS. A nurse short message service by cellular phone in type-2 diabetic patients for six months. J. Clin. Nurs. 2007;16,(6):1082-1087. ![]()
18. Kim CS, Park SY, Kang JG, Lee SJ, Ihm SH, Choi MG and Yoo HJ. Insulin dose titration system in diabetes patients using a short messaging service automatically produced by a knowledge matrix. Diabetes Technol. Ther. 2010;12,(8):663-669. ![]()
19. Yoon KH and Kim HS. A short message service by cellular phone in type 2 diabetic patients for 12 months. Diabetes Res. Clin. Pract. 2008;79,(2):256-261. ![]()
20. Cho JH, Lee HC, Lim DJ, Kwon HS and Yoon KH. Mobile communication using a mobile phone with a glucometer for glucose control in Type 2 patients with diabetes: as effective as an Internet-based glucose monitoring system. J. Telemed. Telecare 2009;15,(2):77-82. ![]()
21. Arsand E, Tatara N, Ostengen G and Hartvigsen G. Mobile phone-based self-management tools for type 2 diabetes: the few touch application. J. Diabetes Sci. Technol. 2010;4,(2):328-336.
22. Dick JJ, Nundy S, Solomon MC, Bishop KN, Chin MH and Peek ME. Feasibility and usability of a text message-based program for diabetes self-management in an urban African-American population. J. Diabetes Sci. Technol. 2011;5,(5):1246-1254.
23. Fischer HH, Moore SL, Ginosar D, Davidson AJ, Rice-Peterson CM, Durfee MJ, Mackenzie TD, Estacio RO and Steele AW. Care by cell phone: text messaging for chronic disease management. Am. J. Manag. Care 2012;18,(2):e42-7.
24. Rami B, Popow C, Horn W, Waldhoer T and Schober E. Telemedical support to improve glycemic control in adolescents with type 1 diabetes mellitus. Eur. J. Pediatr. 2006;165,(10):701-705. ![]()
25. Zolfaghari M, Mousavifar SA, Pedram S and Haghani H. The impact of nurse short message services and telephone follow-ups on diabetic adherence: which one is more effective? J. Clin. Nurs. 2012;. ![]()
26. Farmer A, Gibson O, Hayton P, Bryden K, Dudley C, Neil A and Tarassenko L. A real-time, mobile phone-based telemedicine system to support young adults with type 1 diabetes. Inform. Prim. Care. 2005;13,(3):171-177.
27. Farmer AJ, Gibson OJ, Dudley C, Bryden K, Hayton PM, Tarassenko L and Neil A. A randomized controlled trial of the effect of real-time telemedicine support on glycemic control in young adults with type 1 diabetes (ISRCTN 46889446). Diabetes Care 2005;28,(11):2697-2702. ![]()
28. Franklin VL, Waller A, Pagliari C and Greene SA. A randomized controlled trial of Sweet Talk, a text-messaging system to support young people with diabetes. Diabet. Med. 2006;23,(12):1332-1338. ![]()
29. Turner J, Larsen M, Tarassenko L, Neil A and Farmer A. Implementation of telehealth support for patients with type 2 diabetes using insulin treatment: an exploratory study. Inform. Prim. Care. 2009;17,(1):47-53.
30. Rossi MC, Nicolucci A, Di Bartolo P, Bruttomesso D, Girelli A, Ampudia FJ, Kerr D, Ceriello A, Mayor Cde L, Pellegrini F, Horwitz D and Vespasiani G. Diabetes Interactive Diary: a new telemedicine system enabling flexible diet and insulin therapy while improving quality of life: an open-label, international, multicenter, randomized study. Diabetes Care 2010;33,(1):109-115. ![]()
31. Cole-Lewis H and Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol. Rev. 2010;32,(1):56-69. ![]()
32. Kang BS and Ko IY. Effective route maintenance and restoration schemes in mobile ad hoc networks. Sensors (Basel) 2010;10,(1):808-821. ![]()
33. Kabadi SM, Lee BK and Liu L. Joint Effects of Obesity and Vitamin D Insufficiency on Insulin Resistance and Type 2 Diabetes: Results from the NHANES 2001-2006. Diabetes Care 2012, Epub ahead of print. ![]()
34. Liu L and Nunez AE. Cardiometabolic syndrome and its association with education, smoking, diet, physical activity, and social support: findings from the Pennsylvania 2007 BRFSS Survey. J. Clin. Hypertens. (Greenwich) 2010;12,(7):556-564.
